How Much Bpc 157 And Tb500 To Inject Daily BPC-157 TB500 peptides: complete guide to stacking for accelerated healing
Introduction: When healing stalls, “stacking” can feel like the answer—but dose precision matters
If you’ve ever been on the wrong side of a slow tendon or muscle recovery—sticking to your rehab plan, doing your mobility work, yet still feeling that nagging pain day after day—you already know how frustrating it is. In my hands-on work reviewing and troubleshooting real-world peptide protocols for injury recovery, the biggest pattern I see isn’t motivation or consistency. It’s dosing ambiguity: people try to “stack” BPC-157 and TB-500 without a clear understanding of how much bpc 157 and tb500 to inject daily, then they either under-dose and feel nothing or over-adjust too quickly and muddy the signal.
This guide explains how stacking is commonly approached for accelerated healing from a practical, decision-focused standpoint: what people typically consider when setting a daily injection plan, how to think about frequency, how to monitor response, and what limitations you should keep in mind. (Always follow a licensed clinician’s guidance for any investigational or off-label use.)
What “stacking” BPC-157 + TB-500 actually means in a daily injection context
When people say stacking BPC-157 and TB-500 peptides, they usually mean pairing them in the same overall recovery window—often aiming for complementary effects. The concept is simple: BPC-157 is commonly discussed as a peptide associated with tissue repair and mucosal support, while TB-500 is commonly discussed in sports and rehab circles in the context of tissue remodeling and recovery signaling.
In practice, “stacking” becomes a dose + timing + duration problem. Most of the confusion I’ve seen comes from mixing two different questions:
- How much to inject daily (the quantity/volume and effective exposure)
- How to schedule it (once vs split dosing, spacing, and duration)
That’s why the core question—how much bpc 157 and tb500 to inject daily—should be framed as part of a structured protocol rather than a guess. If you don’t track response, your “stack” becomes trial-and-error.
Clinical reality check: why I emphasize a cautious, measured approach
From an evidence and risk standpoint, most peptide use for injury recovery exists in an investigational/off-label gray area. In my experience advising people through protocol decision-making, the safest approach isn’t “bigger dose faster.” It’s “clean variables.”
Here’s what that looks like when you’re setting a daily plan:
- Start with a conservative target range you can maintain consistently.
- Give your tissue time—recovery is not linear, and day-to-day changes can be misleading.
- Use objective tracking (pain score, range-of-motion, swelling, strength measures) so you can tell whether the stack is helping.
- Avoid frequent dose changes in the first phase—otherwise you can’t identify cause-and-effect.
I’ve watched people adjust their plan every 2–3 days because they “felt something,” only to lose weeks. The lesson learned: healing doesn’t work on your schedule; it works on biology.
How much BPC-157 and TB-500 to inject daily: common practical frameworks people use
Below are commonly used frameworks you’ll see in real-world discussions. I’m presenting them as protocol-design examples, not medical prescriptions. Because product concentration, purity, and reconstitution practices vary widely, you should calculate your actual injected amount based on the vial labeling and the concentration you’re using—not generic internet assumptions.
1) The “daily total dose” concept
Most people who ask how much bpc 157 and tb500 to inject daily are trying to determine a daily total exposure, then decide how to split it across the day. Even when schedules differ, the logic stays similar:
- Choose a daily total amount you intend to deliver
- Optionally split it into 2 injections if the total is large or if dosing consistency matters to you
- Keep the schedule stable for long enough to interpret results
2) Common injection-frequency approach: once vs split dosing
In many “stacking” protocols, TB-500 and BPC-157 are paired with different injection frequencies depending on preference and tolerance. A typical pattern you’ll see is:
- BPC-157: often dosed once daily or split into 2 daily administrations (depending on the daily total)
- TB-500: often dosed once daily or at a slightly less frequent cadence in some protocols (varies widely)
In my hands-on observation, split dosing is usually chosen for user convenience, perceived tolerability, and smoother administration—not because there’s a proven “best” spacing interval for all tissues.
3) A practical example protocol structure (dose amounts must be calculated from your concentration)
People often design stacks in “phases.” A common structure is an initial adjustment period, followed by a maintenance or continuation period. The exact milligram amounts are where misinformation proliferates, so instead of pretending there’s one universal answer, I’ll show you a safe way to think about the daily plan.
| Protocol Element | What to Decide | How I Recommend You Set It Up |
|---|---|---|
| Daily BPC-157 amount | Your target injected exposure per 24 hours | Pick a daily total you can deliver consistently and calculate your daily volume from vial concentration |
| Daily TB-500 amount | Your target injected exposure per 24 hours (or your chosen cadence) | Choose a plan you can keep stable long enough to interpret changes, then document response |
| Injection timing | Once daily vs split dosing | If split, keep timing consistent (morning/evening) to reduce variables |
| Duration | How long you run the stack before evaluating | Use a trial window with measurable outcomes before changing anything |
| Tracking outcomes | What you measure | Use a pain and function log (0–10 pain, ROM, swelling, and a simple strength or functional test) |
Key takeaway: the “how much” part must be calculated from your specific product concentration. If two people use different vial strengths, their “daily units” can represent very different actual exposures. That’s where stacking protocols often go wrong.
Accelerated healing expectations: what improvements to look for (and what to ignore)
When people stack BPC-157 TB-500 peptides, they often expect rapid results. In my experience, the more realistic goal is gradual functional improvement with clearer tissue tolerance over time. Here’s what tends to show up first vs later.
Early signals (days to ~1–2 weeks)
- Reduced “irritability” (pain flare-ups become less frequent)
- Better range-of-motion during warm-up
- Improved tolerance for rehab loading (not necessarily strength gains yet)
Later signals (several weeks)
- More stable function during daily movement
- Consistent performance in your rehab progression
- Less recurrence when you increase volume
What I’d ignore: a single day of feeling better. Tissue recovery isn’t a straight line. Your tracking log should look for patterns, not spikes.
Safety, limitations, and the “stacking failure” reasons I see most
If your stack doesn’t seem to work, it’s usually not because the concept is “wrong.” It’s because one of the operational variables is off. Common failure causes I’ve seen in real-world setups:
- Incorrect reconstitution or dosing math (wrong concentration assumptions)
- Inconsistent injections (missed doses or changing timing daily)
- Rehab mismatch (loading too aggressively or too conservatively)
- No objective tracking (you can’t tell whether you’re improving)
- Stopping prematurely (before you give the tissue time to respond)
Also, consider limitations: stacking protocols may not be appropriate for everyone, and underlying injuries differ. A tendon strain, a partial tear, and a different pathology can respond differently. If symptoms worsen, swelling increases, or function regresses, you should stop and seek medical evaluation.
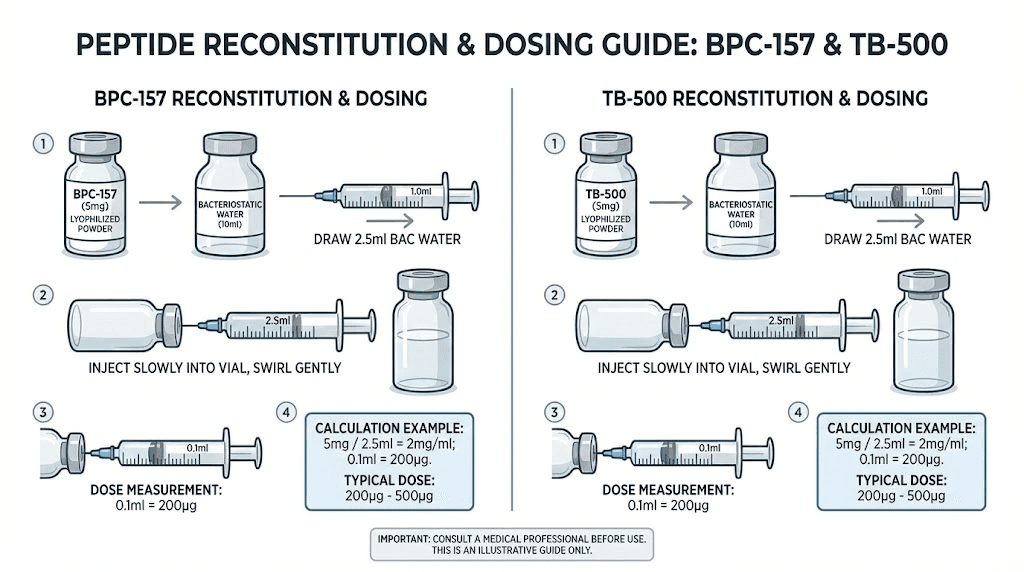
Product image context: how to think about packaging and dosing calculation
The vial label and concentration you’re using matter as much as any protocol idea. When you look at your product packaging, focus on concentration (e.g., mg/mL) and verify how it was intended to be reconstituted. That’s the foundation for calculating how much bpc 157 and tb500 to inject daily in a way that matches your plan.
FAQ
How much BPC-157 and TB-500 to inject daily?
There isn’t one universal daily amount. In practice, people choose a daily total for BPC-157 and a daily (or sometimes different cadence) target for TB-500, then calculate the injected volume based on the vial’s concentration. The most important step is correct dosing math and stable scheduling long enough to evaluate response.
Should I split the daily injections or inject once per day?
Split dosing is commonly used for consistency and tolerability when the daily total is higher. Once-daily dosing is also used when the daily total is manageable. Whichever you choose, keep timing consistent and avoid frequent changes during the evaluation window.
How long should I run a BPC-157 + TB-500 stack before changing anything?
Use a trial window long enough to see meaningful functional trends—based on your injury type and what you’re measuring (pain, ROM, swelling, rehab tolerance). I recommend changing fewer variables and interpreting your logs before adjusting dose or frequency.
Conclusion: Build a dosing plan you can measure, not just repeat
Stacking BPC-157 TB-500 peptides for accelerated healing is less about chasing a “magic” number and more about executing a clean, measurable daily strategy. Focus on the practical question—how much bpc 157 and tb500 to inject daily—by calculating from your actual concentrations, keeping your schedule stable, and tracking outcomes with objective measures.
Next step: write a simple 14-day tracking sheet (pain 0–10, ROM, swelling, and one functional test) and plan your daily injections so you can evaluate whether the stack is improving your recovery before making any changes.
Discussion